What is the ERA Test?
Thank you for finding your way here. My goal is to equip everyone with fertility knowledge no matter where you live.
Whether you’re doing an endometrial receptivity analysis (ERA) or a frozen embryo transfer, this post is for you. Doing an ERA test is like doing everything you would normally do for a frozen embryo transfer cycle except instead of showing up at the lab for a transfer, we remove cells from the uterine lining (the endometrium) to analyze first in my office.
What follows is my process and a step-by-step guide for how I approach the endometrial receptivity analysis (ERA) test with my patients.
Are you ready to dive in? Let’s do it.
Let’s talk about partying. I’m one of those super annoying people that’s always positive. I do this intentionally as I deal with some pretty heavy stuff as a doctor. Therefore I need to have a mindset where I wake up each day full of energy to see my patients and to find solutions to whatever we encounter. I approach the ERA test with the same enthusiasm.
Imagine this scene.

You’ve been invited to a pool party. You show up, and then nobody is there. You feel like a huge dork. It’s either the wrong day or you’re too early…or maybe even too late. Either way, you end up leaving and feeling disappointed. How could you have gotten that wrong?
I think of the ERA test report as the official evite for your embryo transfer. I consider the date and time of your transfer day as possibly one of the most important days of your life. You want to make sure you have the timing right and here’s how.

Your ERA report is the official invitation telling you what time to show up for your embryo transfer party.
On the same day of the ERA test, I like to also do another test too. The Receptivadx test helps you understand the proper attire, or the protocol that’s going to be used for your embryo transfer.
With my patients, I do one endometrial biopsy. I then send tissue to two different companies. One company (Igenomix) tells me the progesterone start time before the transfer day. I know this from the results of the ERA test because it tells me the number of progesterone hours needed for the lining to be receptive and for implantation to occur. Results from the other company (Receptivadx.com) tells me the possibility of there being: inflammation (from endometriosis), infection, possibility of a hydrosalpinx, or microscopic polyps.
All of this is critically important information. It helps me make sure that the lining of the uterus (endometrium) is ready and the protocol is done correctly. Think about the protocol as what you need to wear to the party and your personalized embryo transfer window (ERA result) as the time to show up. This is the one party you want to show up to on time, so that the embryo sticks around for nine months.
I’m a big fan of questions. And so I want to treat this post as a series of questions that I will answer for you.
As always, please review these with your own doctor.
- What is the ERA test?
- What medications will I take?
- How will I feel on the medication?
- How is the ERA test done?
- When can I expect to receive results from the ERA test?
- What will it tell me?
Most of my patients are over the age of 39 and are lucky if they get one or two healthy embryos from an IVF cycle. I am very careful and mindful of everything I do with the embryos. I want everyone to get pregnant. I wish a 100% pregnancy rate was a thing. But of course, it is not.
IVF with genetic testing is the murkiest of all crystal balls, but it’s the best we have. So what can I do as a doctor to help bridge the gap between a less than 100% success rate and a desired 100% success rate? Tests like ERA and Receptivadx help increase our chances of success by giving us more information on how to achieve the best outcomes.
The time to talk about these tests for me isn’t after a failed transfer. Certainly, there are doctors that talk to their patients about these types of tests after a failed transfer. I prefer for my patients to know about them ahead of time. Then you have the choice to do the tests or not. I don’t want my patients to experience any regret if I can help it.
Here’s the thing. Some people think these tests are only for patients that have never been pregnant. Even if you have had a successful pregnancy you should still consider these tests. The reason is this: The ERA Test doesn’t tell us if you “can” or “can’t” get pregnant. It just guides us along the lines of how to best approach your transfer.
I help my patients make the decision if they should do these tests based on their answers to these questions:
How many embryos do they have?
What have they been through before? For example, how many transfers
How many kids do they want?
I also do these tests on people who have gone through donor egg IVF and on first time surrogates. Once you get to the point of using a surrogate, most patients have been through so much that success matters more than ever. This is why it makes sense to do this test before a frozen embryo transfer for a first time surrogate too. I don’t consider doing this test on a repeat surrogate because their previous medication protocol is in a way their ERA test because I just mimic what they were on before.
What is an ERA test?
This is an example of what the results look like. The results show that the uterine lining is receptive after being on progesterone for 131 hours leading up to the test day.
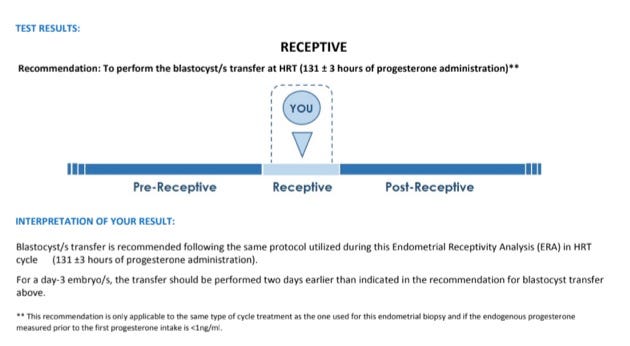
So what does this mean?
The ERA is a test that analyzes genes within the lining of the uterus. We remove cells from the lining of the uterus through an endometrial biopsy procedure. Here are a few important tips:
- When the weather is really warm, make sure your center knows how to package the sample properly so the sample isn’t affected by extreme temperatures
- Be sure that your doctor doesn’t use any iodine/anti-septic in the vagina before performing the biopsy. If the cells are contaminated, the DNA can’t be extracted from the tissue
- If your doctor wants to do a saline sonogram or hysteroscopy, do it after the biopsy is taken because the fluid used can contaminate the cells.
The cells are placed in a small container and sent to the genetic testing company where next-generation sequencing is performed. This means that genes responsible for implantation are analyzed. We know that these genes are expressed after a certain number of hours of progesterone and this number varies from uterus to uterus. Based on the results, we can tell how many hours of progesterone a woman needs in order for her lining to be receptive to an embryo. We call this the window of receptivity. That window is approximately 24 hours.
This test does not tell us what day to do the transfer. I can still pick my transfer day. What this tells me is how many hours backward from the transfer day to start progesterone.
So for this patient, we pick the transfer day and then calculate backward 131 hours. For this patient that’s the exact time they will start progesterone. I use this website to calculate everything.
I like to be exact so that I can go to sleep at night knowing that I did everything possible for a patient to get pregnant. I want to give every embryo their best chance at implanting.

What medications do you take?
The goal behind taking medications is to mimic the hormonal changes that occur during ovulation. We use hormones (estrogen and then estrogen and progesterone combined) to make sure that the uterus is ready and synced up with the embryo around the same time implantation would naturally occur after ovulation. We start with estrogen starting cycle day #2 (the day after your period starts). Estrogen is secreted by the ovaries when we ovulate. Estrogen levels rise slowly during the cycle. After ovulation, progesterone levels rise. We use two weeks of estrogen and then the third week we combine with progesterone. We have different options for estrogen: pills, patches, or shots. If you’re someone that may forget to take a pill then either the patch (dosed every 2 days) or the shot (dosed every 3 days) may be best for you.
Most people hear shot and don’t want a shot. In that case, we go for estrogen pills. (Often call estradiol). We take them twice a day. They are little blue pills. Take two in the morning and two at night. I like to give my patients instructions. Pick an hour (8AM and 8 PM) and stick to a schedule. If you don’t take them exactly 12 hours apart, then you may ovulate. These medications take over your cycle and suppress ovulation. So one of the things you can do is have sex and not worry. There’s no need to abstain. Sometimes when you go through all of the work of creating an embryo you may be concerned about getting pregnant in the middle of the process. Of course, pregnancy is the goal so it’s not something to fear, but it’s worth noting that you will not be able to become pregnant via intercourse while on these medications.
I also recommend prenatal vitamins and aspirin (not time sensitive). I want to reduce the risk of blood clots while taking estrogen as this is a potential risk. It’s a low risk, but I still like to eliminate any complications by asking my patients to take a small dose of aspirin each day.
How will you feel on the medication?
All hormones have side effects. Talk to your doctor about what you can expect. Since the meds are used to mimic ovulation, you may feel like you’re ovulating. You may experience: breast tenderness, egg white cervical mucus, and you may get headaches or feel a little nausea. Keep your doctor in the loop about how you’re doing. Depending on how you feel, medications can be adjusted to help manage your symptoms.
For example, one of my patients called me to say the medications were making her feel like a “crazy” person. I asked her to tell me exactly what her symptoms were, we then figured out a way to make adjustments to address them. One of the things you can do is modify the dose and or frequency of meds. Decreasing the dose to one tablet three times a day, or one tablet vaginally twice a day may help. Although I have to warn you that you may develop what I call, “smurf vagina” or “smurfgina.” Think about it…the tablets are blue and you’re placing them in your vagina. Okay. I’m done. That’s my joke for the day.
You can also do the test during a natural cycle in which you monitor follicle growth by ultrasound and induce ovulation with an HCG injection, then do the biopsy 7 days later. I offer this approach to women who either don’t feel well on estrogen or in women who make a better lining during a natural cycle’s ovulation.
How is the test done?
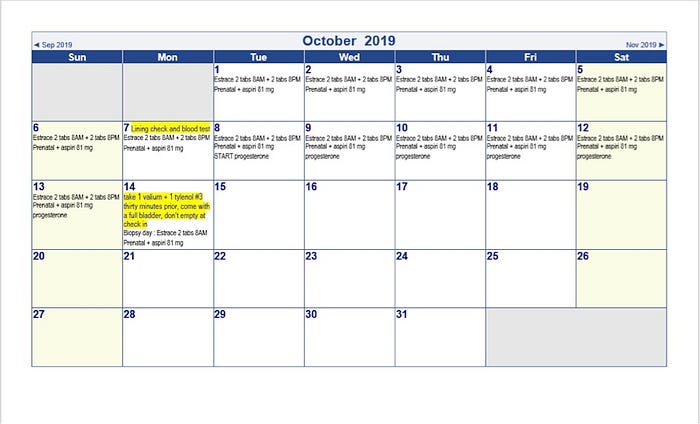
The test isn’t as simple as doing a blood test. After two weeks of taking the medication, you come in for a lining check and blood test to monitor your progesterone. We want to make sure that your lining thickness is between 9–12mm and that your progesterone is low.
It’s not just about the thickness it’s also about the texture. Sometimes a patient’s thickness is slightly less than 9 or more than 12. That’s okay. In general, we want the 9–12 range and a progesterone level that’s barely detectable or less than 1. If the lining isn’t thick enough, I may increase the dose of estrogen and have the patient come back a week later before starting progesterone.
Once the lining is thick enough, I then make sure to review progesterone options with my patients. There are several options for progesterone. The theme is vaginal inserts or injections of progesterone in oil . On very rare occasions I’ve used only oral progesterone for cycles like this, but it was only because the patient had severe reactions to the other types.
With the vaginal inserts, I reinforce the importance of timing. If you skip one the pregnancy could be done. When you use a progesterone shot it’s an oil so there’s a build-up in your system. When you’re using vaginal progesterone there isn’t the buildup so you reliably have to place the insert three times a day.
I give my patients very specific instructions. 8AM, 2PM, 8PM. On the dot. This is a good test to see if you can take your medications on time and never skip one. Consider setting phone alerts, have someone call you and ask, “Did you put the tablet in your vagina?” Ha, whatever it takes! Imagine how fun that call will be to get.
With the progesterone shots, I’m telling you —be prepared. These things hurt like heck.
I’m going to share my tips for taking the progesterone injection. I use progesterone compounded in ethyl oleate 100 milligrams per ml. This is concentrated as a double-strength dose so that patients don’t have to take two ml but just one. My preferred dose is 100 milligrams, but talk to your doctor as every doctor is different.
After you draw up the medicine, put it under your armpit. (Make sure you’ve showered — ha.) Keep it there just to warm it a bit. I’ve seen people do things like put the vial in the microwave. Don’t ever do that. As you’re warming it under your arm put an ice pack on your butt. After you’ve drawn it up with the 18G needle, switch to the 25 G needle (1 inch for smaller frames, and 1 1/2 inch needle for larger frames). Insert the needle all the way, pull back a touch on the plunger to make sure you’re not in a vessel, inject, then withdraw. Dab with a little gauze if there’s any leakage of oil or blood. Have someone give you a nice butt massage. Consider using a heating pad as well as a handheld vibrating massager to massage the injection sites. These steps may help make the shot less painful.
You’re only going to do the injections for six days of the mock cycle. I also call this an implantation testing cycle or rehearsal cycle. During the real deal, you‘re going to be taking progesterone through 10 weeks of pregnancy. If you’re doing a blastocyst transfer, you are considered almost 3 weeks pregnant on your transfer day. A little over seven weeks later you’ll be done with the shots. You can consider taking the shots during the week when you’re working and then switch to inserts on Friday, Saturday, and Sunday nights to give your butt a break. There are lots of things you can do to make your butt less sore as you’re going through this process (ice, heat and massage and anti itch cream if you start to feel itchy over the injection site).
When will you get results back?
After the biopsy is done you get results back about two weeks later. The good news is that you don’t need your results back until you do your next lining check. This way, you can still start meds cycle day #2 of the period that starts 3–5 days after the biopsy. Once you get the results back, you know exactly when to start progesterone before your transfer. One of the most common questions I get asked after the procedure is, when can I transfer? And the answer is that as soon as your period starts after you stop your hormones from the time of the biopsy, you can restart your meds and transfer 3 weeks later. The number of days of estrogen isn’t important to reproduce exactly from the ERA test cycle protocol. We are doing this test to learn about when to start your progesterone. Another important thing to know: You can also do the test and wait until you’re ready to transfer at a later time. You don’t have to transfer right away after the test. The results are good for up to 3 years. I also sometimes repeat the test for patients coming back for another pregnancy with me.
What will the test tell you?
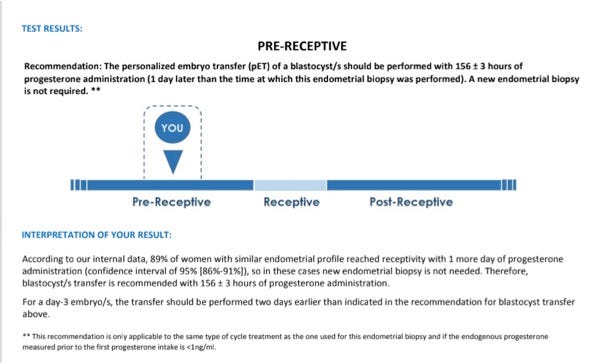
This sample report above is giving us a result of 156 hours. In general, my patients are receptive at around 134 hours. Thank goodness we have this tool so I know when to show up to the embryo transfer party. I feel really confident in my ability to design an individualized embryo transfer protocol for each patient.
I use this personalized embryo transfer calculator to set up each transfer calendar after I get the ERA test report.

It’s pretty simple. You fill in the information you learn from your doctor: when you’re going to transfer, the ERA results (number of hours of progesterone), and then it will tell you exactly what day and time to start the progesterone.
Before we wrap this topic I want to talk about the actual way we get tissue for these implantation tests: an endometrial biopsy.
After placing a speculum, I use a small plastic catheter (called a pipelle) to extract cells attached to the wall of the uterus. Patients are sometimes scared that the transfer will feel the same as the biopsy. I promise you it won’t. When I do the transfer I am pushing microscopic cells into the uterus with the transfer catheter. This isn’t a painful procedure.
I don’t believe in causing patients pain. I try and think of myself as the pain-free fertility doctor. I wish it could be pain-free, but I really do my best. The internet makes this test sound awful. I don’t want it to be awful nor should it be. For that reason, I offer all of my patients a valium and a Tylenol with codeine thirty minutes before the procedure. I ask patients to come into the office with a full bladder. Having a full bladder not only allows me to see the uterus under abdominal ultrasound guidance if needed but it also helps the uterus lean back allowing a straight path for the pipelle. I also make sure they eat ahead of the appointment so they aren’t super dizzy from the pain meds. Lastly, please arrange to have someone drive you.
I want patients to not remember their endometrial biopsy as the most painful experience of their lives. I tell patients that I’m going to count to five and their pain score is going to go from zero to eight during that five-second interval. After I remove the pipelle the pain level will be at a six. About ten minutes after that it will be at a three out of ten. Within twenty minutes it will be at a zero. After the procedure, you can empty your bladder. I also sometimes do this procedure with a saline infusion sonogram or under anesthesia when I also want to do a hysteroscopy or if a patient has a very low pain threshold.
Going through implantation testing helps with several things:
- A mock embryo transfer. This will guide the doctor on how to place the transfer catheter.
- Serves as a guide for the transfer protocol and progesterone timing.
- It helps you see how you feel on the medications so you can adjust things as needed for the real transfer. For example, if you have a reaction to a medication it’s best to know this before the real transfer.
Think of it as a dress rehearsal for the actual performance.
In Summary:
If you haven’t watched this show, How to Get Pregnant in 3 Months or Less, I highly suggest you do. Or encourage you to read the blog post here.
I’ve covered a lot of things here that relate to the second month of how to get pregnant in three months or less. This was the break down of that second month for you.
I really hope this is helpful no matter who you are or where you live. I have been doing implantation testing since 2013 and find it helpful. Take these six questions to your doctor so that you can learn more about the test and how it may help you.
- What is the ERA test?
- What medications will I take?
- How will I feel on the medication?
- How is the ERA test done?
- When can I expect to receive results from the ERA test?
- What will it tell me?
As always, please send me a note, email@eggwhisperer.com, if you have any further questions or you’d like to recommend a topic for a future show.
You can also catch more of me and topics like this through The Egg Whisperer Show. The episodes are live-streamed on YouTube, Facebook, and Twitter and on Wednesdays at 7 PM PST. Subscribe to the podcast too!
